Mandible (Lower Jaw Bone)
Published on February 7th 2022 by staff
What is the Mandible
The mandible is the largest, strongest, and the only skull bone capable of movement. It forms the lower jaw, and thus is also known as the lower jaw bone. It helps with the process of chewing along with the maxilla or upper jaw bone.
The bone has derived its name from the Latin word ‘mandibula’, which is derived from ‘mandere’, meaning ‘to chew’, and ‘bula’, an instrumental suffix.
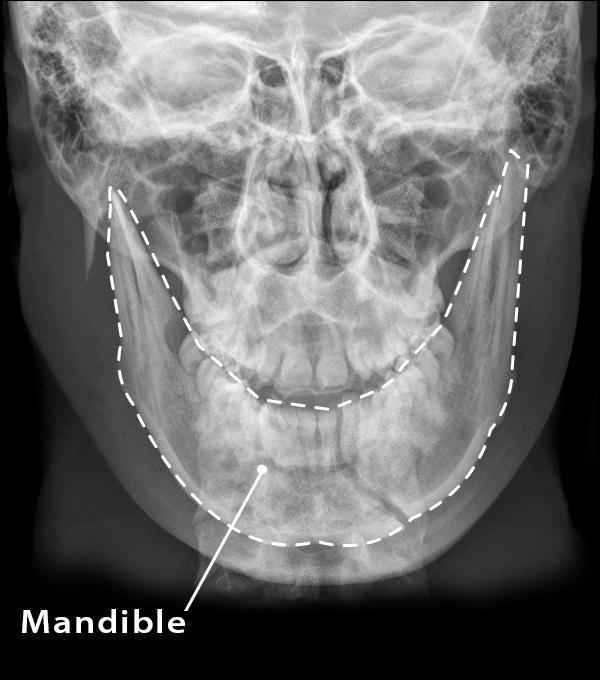
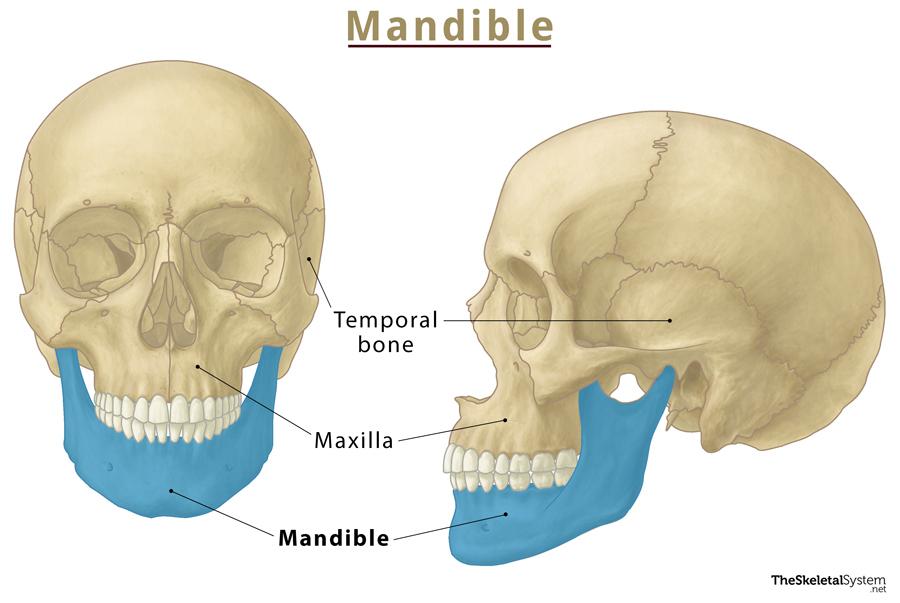
Where is the Mandible Bone Located
As stated, the mandible is located in the lower jaw, just inferior to the maxilla or upper jaw. You can easily feel the bone by touching your lower jawline.
Quick Facts
| Type | Irregular bone |
| Length | In males: Approximately 17-19 cm In females: Approximately: 16-18 cm |
| How many are there in the human body | 1 |
| Articulates with | Temporal bone |
Functions
- Forms the lower jawline, shaping the face and chin. The teeth in the lower jaw are also rooted to this bone.
- Helps in mastication or chewing of food.
- Being the only mobile skull bone, it aids in the movement of the mouth, helping with eating, and talking.
- Forms and protects the organs and vessels in the oral cavity.
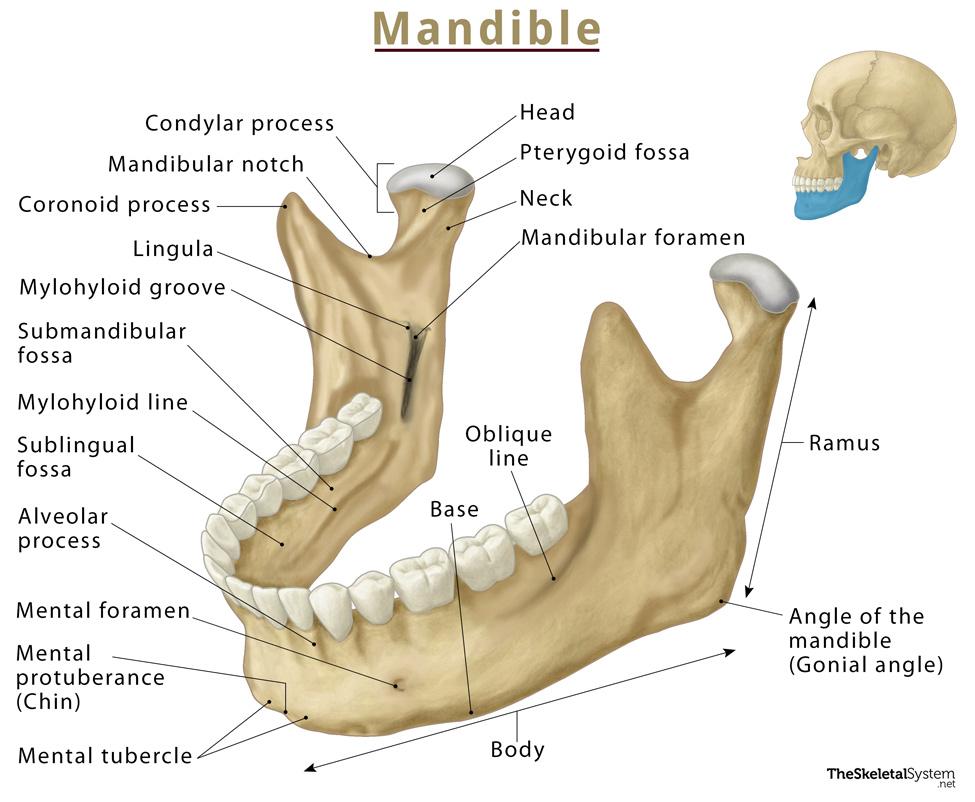
Parts and Anatomy of the Mandible
It is a single, horseshoe-shaped bone consisting of a horizontal body on the anterior side and two vertical rami on the posterior side.
Body
The body is curved, having two borders and two surfaces.
Borders
The superior border is called the alveolar border, whereas the inferior one is the base.
Alveolar Border (Superior): An essential bony landmark, the alveolar process extends superiorly from this border. It comprises two bony plates: a thick buccal and a thin lingual. This is the most vital region of the mandible, as it holds 16 sockets or cavities for the lower set of teeth. Each side of the mandible holds 5 primary teeth and 7-8 permanent teeth.
Base (Inferior): It is the lower border of the bone, where the digastric muscle attaches medially. It also provides a small groove through which the facial artery passes.
Surfaces
The part of the bone facing the oral cavity is the inner surface, whereas the one facing outwards is the outer surface.
Inner Surface: On the medial side of the inner surface, there are some important structures, including the superior and inferior genial tubercles or mental spine, digastric fossa, and mylohyoid line. The mylohyoid line divides the mandible into submandibular and sublingual fossae, where the two salivary glands, submandibular and sublingual, rest. The pterygomandibular raphe attaches to the posterior border of the mylohyoid line.
The internal surface contains the median ridge at the midline and mental spines, which are just lateral to the ridge. The mylohyoid line begins at the midline and courses superiorly and posteriorly to the alveolar border.
Outer Surface: On the lateral sides of the outer surface, external oblique line, mandibular symphysis, and mental foramen can be seen.
Mandibular symphysis is a bony landmark present in the midline of the mandible. It is a small bone ridge representing the fusion of the two halves during development. Laterally to the ridge and below the incisive teeth, there is a depression known as the incisive fossa. The symphysis encloses a triangular eminence called the mental protuberance, which forms the characteristic shape of the chin. The edges of the mental protuberance are elevated, forming the mental tubercle.
Ramus
As mentioned, the bone features two mandibular rami (singular: ramus) that project perpendicularly upwards from the angle of the mandible. The body and the rami meet on each side at the angle of mandible or gonial angle. This angle can range from 110-130 degrees and vary depending on age, sex and ethnicity.
At the superior point, the ramus divides into two processes, the coronoid process on the anterior side and the condylar process on the posterior side. A mandibular notch separates these two processes.
Head: It is situated posteriorly and articulates with the temporal bone, forming the temporomandibular joint.
Neck: It supports the head of the ramus and also acts as a site of attachment for the lateral pterygoid muscle.
Coronoid Process: It is located on the superior side of the ramus. The temporalis and masseter muscle that helps in chewing attaches to its lateral surface. The anterior border of this process is continuous with that of the ramus, and its posterior border makes the anterior boundary of the mandibular notch.
Condylar Process: It is also located at the ramus’s superior side and divided into neck and condyle. The neck is a slender stalk-like structure projecting from the ramus. There is a protuberance on the top of the neck, the condyle that forms the lower bony component of the temporomandibular joint, along with the temporal bone. The anteromedial surface of the condylar process has a small depression called the pterygoid fovea or pterygoid fossa, where the lateral pterygoid muscle attaches.
Foramina
The mandible is marked by two foramina:
1. Mandibular Foramen
The inner medial side of the ramus contains the mandibular foramen, through which the inferior alveolar nerve and inferior alveolar artery pass. These neurovascular structures travel through this foramen into the mandibular canal and exit at the mental foramen. At the anterosuperior side of the mandibular foramen, there is a sharp process called the lingula of the mandible. Similarly, at the posteroinferior aspect of the foramen is the mylohyoid groove, through which the mylohyoid vessels run.
2. Mental Foramen
The outer surface of the mandibular body contains another foramen, called mental foramen. It is located lateral to the mental protuberance, below the second premolar, and houses the inferior alveolar nerve and artery that exit through the mandibular canal. When the inferior alveolar nerve passes through the mental foramen, it becomes the mental nerve that innervates the skin of the lower lip and the front part of the chin.
Muscle and Ligament Attachments
Muscles originating from the mandible
- Mentalis: From the incisive fossa
- Depressor labii inferioris: From the oblique line
- Orbicularis oris: From the incisive fossa
- Digastric anterior belly: From the digastric fossa
- Depressor anguli oris: From the oblique line
- Buccinator: From the alveolar process
- Mylohyoid: From the mylohyoid line
- Geniohyoid: From the inferior portion of the genial tubercle
- Genioglossus: From the superior portion of the genial tubercle
- Superior pharyngeal constrictor: From the pterygomandibular raphe
Muscles inserted into the mandible
- Platysma: On the inferior border of the mandible
- Deep masseter: On the lateral surface of the ramus and angle of the mandible
- Superficial masseter: On the lateral surface of the ramus and angle of the mandible
- Inferior head of the lateral pterygoid: On the condyloid process
- Medial pterygoid: On the medial surface of the mandibular angle and ramus of the mandible
- Temporalis: On the coronoid process
One important ligament attachment of the bone is that of the sphenomandibular ligament.
Articulations
The mandible is the only bone that doesn’t articulate with its adjacent skull bones with the help of sutures. It forms only one articulation:
Temporomandibular Joint: The condyle part of the condylar process articulates with the temporal bone, forming the temporomandibular joint with the help of the articular disk.
It is attached to the maxilla through muscular and articular attachments, though there is no articulation between them. The only time the two are connected directly is when the upper and lower teeth meet when the mouth is closed.
Ossification and Development
Ossification of the mandible starts during the sixth week of intrauterine development. It is the second bone to ossify.
The first pair of the pharyngeal arch, or the mandibular arch, gives rise to the left and right Meckel cartilage, which serves as a template for the development of the bone. A fibrous membrane covers this cartilage at their ventral ends. From each of the left and right cartilage arises an ossification center. These two halves eventually fuse via fibrocartilage at the mandibular symphysis. As a result, the mandible is still composed of two separate bones at birth.
Ossification and fusion of the mandibular symphysis occur during the first year of life, resulting in a single bone. The remaining part of the mandibular symphysis remains present as a subtle ridge at the midline of the mandible.
The mandible constantly changes throughout an individual’s life. At birth, the gonial angle is approximately 160 degrees. By age four, teeth begin to form, which causes the jaw to elongate and widen. These changes in the mandible’s dimensions cause the gonial angle to decrease to approximately 140 degrees. By adulthood, the gonial angle gets decreased to approximately 120 degrees.
FAQs
Ans. The lateral pterygoid muscle depresses the mandible, whereas the posterior fibers of the temporalis muscle retract it.
Ans. Generally, in males, the angle of the mandible is curved outwards, leading to a sharper angle at the jaws. Females often lack this outwards curving and have a more rounded jaw. In some females, the angle may even invert towards the midline.
References
- The Mandible – Teachmeanatomy.info
- Anatomy, Head and Neck, Mandible – Ncbi.nlm.nih.gov
- Mandible – Radiopaedia.org
- Mandible – Kenhub.com